Incorrect diagnosis codes, undercoded E&M levels, unbundled procedures, and unsupported specificity cost providers an estimated $262 billion in lost or delayed revenue every year. Healthcare Logic's certified coders work from clinical documentation to capture every legitimate dollar — accurately, compliantly, and on time.
Undercoding leaves legitimate revenue uncaptured. Overcoding creates compliance liability and audit exposure. Coding errors trigger denials that cost $25 each to rework. And poor documentation specificity leaves money on the table that your clinical team earned and documented — just not coded correctly.
Studies published in the Journal of the American Medical Association and MGMA benchmarks consistently show that 40% or more of medical practices systematically undercode evaluation and management (E&M) visits. A single level of E&M undercoding across a 3-physician practice can represent $90,000–$140,000 in uncaptured annual revenue.
ICD-10-CM has over 70,000 codes, and payers use automated claim editing systems that reject claims when diagnosis codes lack the specificity required for the billed procedure. An unspecified code where a specific one exists can result in an immediate denial, delay payment by 30–60 days, and occasionally cause permanent write-off.
The AMA releases CPT updates annually, with new, deleted, and revised codes effective January 1. In 2023 alone, over 400 CPT changes took effect. In-house staff who haven't completed annual coding education routinely bill deleted or incorrect codes for months, accumulating denials and compliance exposure.
The most common root cause of coding inaccuracy is not the coder — it's the clinical note. When documentation is vague or incomplete, even the most experienced coder cannot assign the correct code without querying the provider. Without a formal Provider Query process, documentation gaps cause perpetual undercoding.
* Estimates based on JAMA, MGMA, and AAPC benchmarks for a multi-provider ambulatory practice. Healthcare Logic provides a free coding audit to quantify your actual coding gap.
Healthcare Logic provides full-spectrum medical coding for physician practices, FQHCs, hospitals, and health systems — with certified coders, documented specialty training, and a pre-submission audit layer that catches errors before they become denials.
Our coders assign ICD-10-CM diagnosis codes to the highest level of specificity supported by clinical documentation — capturing laterality, acuity, episode of care, and complication codes that payers require for payment. We query providers when documentation falls short of required specificity.
E&M coding is the highest-value coding function for most practices, and the most consistently undercoded. We apply 2023 AMA E&M guidelines using medical decision-making or total time, and review documentation for all elements required to support the level billed.
We assign CPT procedure codes for all service types with explicit attention to NCCI bundling edits, modifier application, and payer-specific coding policies. Modifier 25, 59, 51, and global period rules are applied consistently and documented for payer audit defense.
HCPCS Level II codes are required for supplies, injectable and infused drugs, durable medical equipment, prosthetics, and orthotics. Our coders assign HCPCS codes with the correct units, modifiers, and NDC numbers for drug billing, preventing denials for missing or incorrect data.
We conduct both prospective audits (before submission, for high-risk specialties) and retrospective audits to identify accuracy, specificity compliance, and revenue leakage. Audit results include quantified recovery estimates, coder-level error reports, and provider documentation pattern analysis.
When documentation cannot support accurate coding, our coders generate AHIMA- and ACDIS-compliant provider queries — formal, non-leading requests for clarification. Over time, query patterns identify systemic gaps, enabling targeted education that improves note quality at the source.
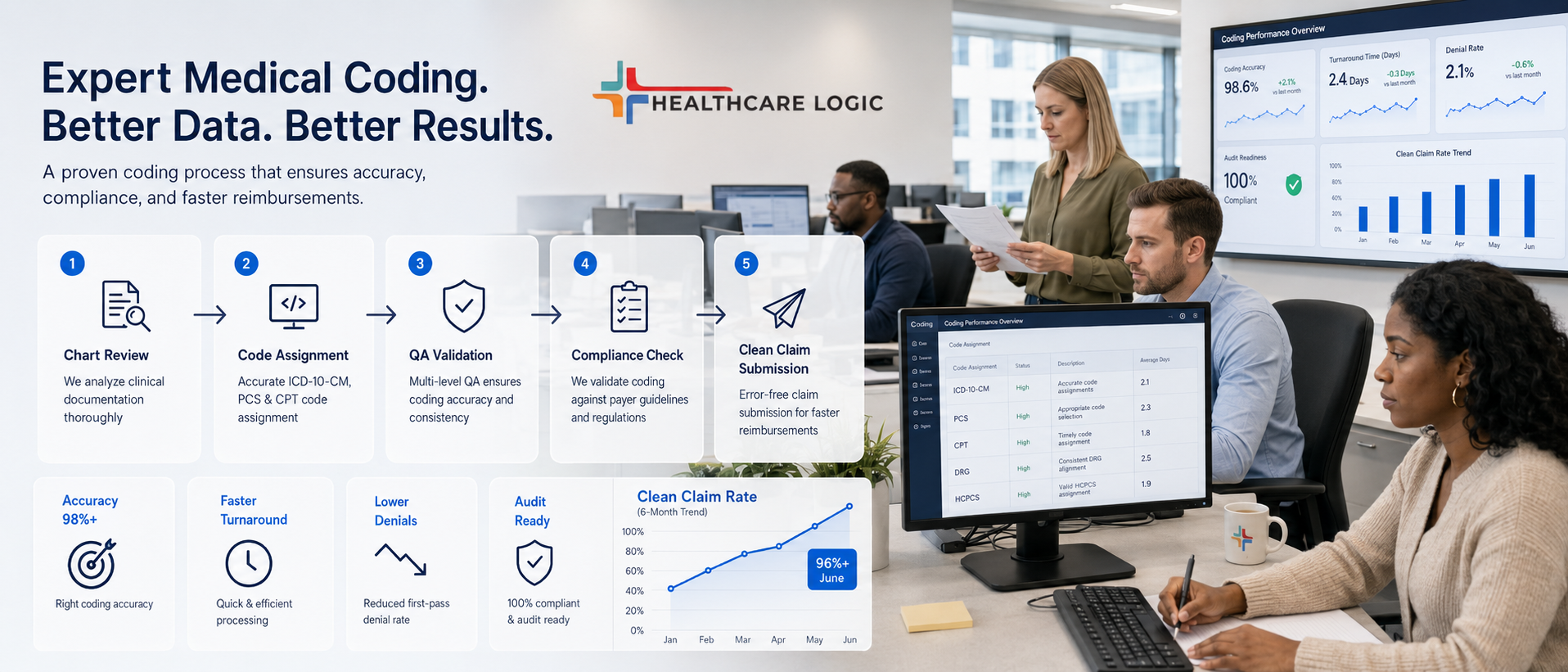
A five-stage medical coding workflow — from documentation receipt to billing-ready code output — built for accuracy, speed, and compliance at every step.
Healthcare Logic's medical coding team combines active credentialing, specialty-specific training, and a documented compliance framework — so every code we assign can be defended in a payer audit, a RAC review, or an internal compliance investigation.
All coders hold active AAPC or AHIMA credentials and complete annual continuing education to maintain certification and stay current with code set updates.
Every code set is cross-validated against CMS NCCI edits, Medicare LCDs, and major commercial payer policies before submission — catching edit-triggering combinations before they reach the payer.
Coders are assigned to your specialty, not rotated through a general pool. Cardiology encounters are coded by cardiology coders; behavioral health by behavioral health coders. Accuracy improves when coders know the clinical context.
Clean claims rate, coding-related denial rate, E&M level distribution, query resolution rate, and coder accuracy scores are reported monthly in your Logic Analytics dashboard.
Each specialty has its own coding ruleset, documentation requirements, and payer policies. Healthcare Logic assigns coders with documented specialty training to every client — not generalists coding across every service line at once.
Healthcare Logic's free coding audit analyzes your E&M level distribution, coding-related denial rate, and ICD-10 specificity patterns — and quantifies the revenue you're leaving behind. No obligation. Results in 5 business days.
Request Your Free Coding Audit Revenue Cycle
Revenue CycleAmbulatory Surgery Centers (ASCs) navigate a complex financial landscape characterized by the Hybrid Billing T...
 Radiology
RadiologyIs your ASC’s revenue cycle moving as fast as CMS? The Covered Procedures List (CPL) Shift...
 Radiology
RadiologyWhen a women’s imaging center or radiology practice upgrades its digital mammography...
